

GLP-1s: Is the absence of craving the same as contentment?
On deciding whether to try them, the brain science of craving, and why wanting less isn't the same as being better.

Is the absence of craving the same as contentment?
That’s the question I keep coming back to every time I read another profile of someone who lost forty pounds on a GLP-1 and then, almost as an aside, mentions they also stopped wanting wine. And shopping. And the 2am spiral of should-I-or-shouldn’t-I. The food noise went quiet, and then, a little more quietly, so did everything else.
The science on this is genuinely interesting and genuinely incomplete, which is how most useful science tends to be. GLP-1 receptor agonists, semaglutide and tirzepatide specifically, don’t just talk to your stomach. They communicate with the brain’s reward circuitry. Nora Volkow at the National Institute on Drug Abuse has spent decades mapping exactly these dopaminergic pathways, the ones that make you reach for another glass, refresh the feed, text back too fast. GLP-1s modulate wanting itself. And they do it, from what the early data suggests, quite well.
Which should probably give us a moment’s pause.
I’ll say where I sit in this, since it’s relevant to the argument. I’ve been trying to answer this question for myself. Not academically. Personally. Sitting with whether to try them. And there’s a view I’ve arrived at that I find mildly inconvenient: if you work in this space and you haven’t tried the thing you’re forming strong opinions about, that’s a gap worth being honest about. Especially if you’re a doctor (which i’m clearly not!). The n=1 data point you’re missing is your own, and that tends to show up in the quality of the thinking.
So I remain curious, genuinely. And equally unsettled. Not by the mechanism. By the category. The idea of getting hooked on a pharmaceutical solution to maintain something I’d always understood as being about will, desire, the kind of person you are. That framing runs deep. Replacing it with a weekly injection feels less like an answer and more like a sharper version of the original question.
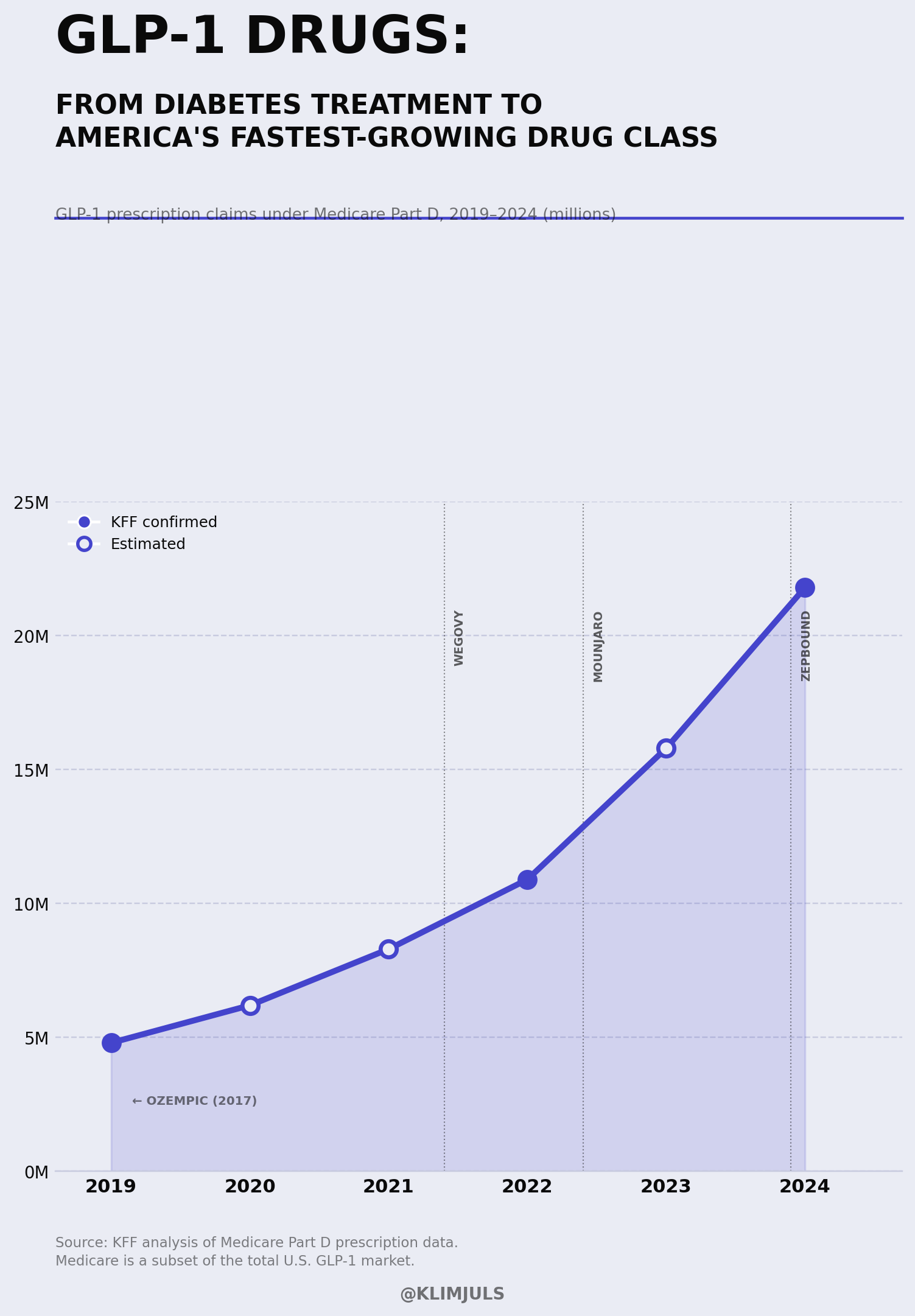
The premium wellness market spent decades building a very expensive infrastructure around a single idea: that craving was the problem. Too much appetite, too much indulgence, too much noise. GLP-1s are the logical conclusion of that project, delivered once weekly, subcutaneously, elegantly.
But here’s the thing. Desire is also, inconveniently, what gets things made. The longing that drives creative work. The hunger that makes someone call the person, stay in the argument, order the dessert and mean it. I’m not making a case against the drugs. That would be facile and also not my lane. I’m making a case for noticing what we’re framing as the problem.
Because when “decreased interest in reward-seeking behavior” is listed as a side effect with quiet neutrality, we’re describing something more than a reduced appetite at dinner. We’re describing a modulation of how a person moves through the world. Research from Olivia M. Farr and colleagues in Diabetologia established that GLP-1 receptors exist in the parietal cortex and hypothalamus — brain regions with nothing to do with digestion and everything to do with how we process experience. A 2025 clinical review by Tveit and colleagues went further: GLP-1s increase serotonergic activity at the 5-HT2C receptor, the same pathway behind SSRI-induced motivational blunting and reduced sexual desire. The mechanism for quieting desire isn’t just theoretical.
The broader psychiatric picture is net positive and I want to be clear about that. Large population studies find GLP-1s associated with meaningful reductions in psychiatric hospitalization, not increases. This is not a story about a drug making people worse in the ways medicine knows how to measure.
What medicine isn’t measuring yet is this: those trials track hospitalization, adverse events, depression scales. They are not tracking whether someone stopped wanting to call the person, lost the pull toward the project that used to wake them up at 6am, or found the things they used to hunger for simply quieter than before. Those don’t register in any database. They’re the texture of a life. And they may be exactly what the 5-HT2C pathway is modulating.
The question isn’t whether these drugs work. They do. The question, and I think it’s the more interesting one, is what we believed was broken that made us reach for them in the first place.
We are all in search of something. That’s the whole premise. But it’s worth asking, occasionally, whether we’re searching for less wanting, or for wanting the right things.
If you’re not subscribed yet:
In Search Of covers the intersection of longevity science, culture, and the questions the industry isn’t asking loudly enough. No hype. No supplement stacks. Just rigorous thinking on what it actually means to build a longer, better life.
→ Subscribe below. One post a week.
References
Farr, O.M. et al. (2016). GLP-1 receptors exist in the parietal cortex, hypothalamus and medulla of human brains and the GLP-1 analogue liraglutide alters brain activity related to highly desirable food cues in individuals with diabetes: a crossover, randomised, placebo-controlled trial. Diabetologia, 59(5), 954–965. PMID 26831302
Volkow, N.D. & Koob, G.F. (2015). Brain disease model of addiction: why is it so controversial? Lancet Psychiatry, 2(8), 677–679. PMID 26249284
Volkow, N.D. et al. (2025). GLP-1R agonist medications for addiction treatment. Addiction. doi:10.1111/add.16626
Tveit, M. et al. (2025). Clinical review of how glucagon-like peptide-1 agonist obesity medications decrease sexual desire, and a biopsychosocial model for why we don’t ‘see’ it. The Journal of Sexual Medicine, 22(Suppl 1). PMC12704374
Sa, B. et al. (2026). Psychiatric effects of GLP-1 receptor agonists: a systematic review of emerging evidence. Diabetes, Obesity and Metabolism, 28(1), 50–59. PMID 41126551
Taipale, H. et al. (2026). Association between GLP-1 receptor agonist use and worsening mental illness in people with depression and anxiety in Sweden: a national cohort study. The Lancet Psychiatry. PMID 41862258
Watabe-Uchida, M., Eshel, N. & Uchida, N. (2017). Neural circuitry of reward prediction error. Annual Review of Neuroscience, 40, 373–394. PMID 28441114
The 5-HT2C mechanism deserves more attention in how we counsel patients. “Decreased interest in reward-seeking behavior” is listed in clinical language as if it is comparable to mild nausea. It is not. It is a qualitative change in how a person experiences daily life, and we do not have good tools for measuring it or even asking about it.
From the pharmacy side, this piece names something we are not accounting for in coverage decisions either. Utilization management criteria for GLP-1s are built around BMI thresholds and comorbidities. Nobody is asking whether the patient’s experience of motivation and desire fundamentally changed, because that is not a metric. Patients are reporting it consistently enough that the pattern deserves a more honest clinical conversation than “the benefits outweigh the risks
I am also fascinated by the “flattening of life” side effects. For my latest piece, the six folks I interviewed hadn’t experienced it…but I still wonder how dampening hunger would not also dampen other desires! Need to do more research, thank you for this piece.